Schizoaffective disorder combines features of schizophrenia with mood disorder symptoms like depression or mania. It affects approximately 0.3% of the American population, about 3 individuals out of every 1,000. According to a study published in Yale Medicine titled “Schizoaffective Disorder.”
Key signs of schizoaffective disorder include mood swings, which vary from extreme highs to severe lows, as well as disorganized thinking that affects clarity and coherence in speech and thought processes. People also experience social withdrawal, distancing themselves from friends and family, and exhibiting a general decline in social engagement.
The causes and risk factors for schizoaffective disorder disorder include genetics, neurobiological factors, and environmental influences, such as trauma or stress. To diagnose schizoaffective disorder, the psychiatrist implements a comprehensive evaluation of symptoms, and medical history, and rules out other mental health conditions.
Treatment options for schizoaffective disorder involve antipsychotic medications, mood stabilizers, and psychotherapy, which effectively reduce symptoms and improve quality of life. Art therapy also provides valuable opportunities to develop new ways of connecting with others, express your emotions, accept your feelings, and gain insight into your emotional state, per a research published by Mental Health UK titled “Treatments for schizoaffective disorder.”
The prognosis for this disorder varies, with some individuals achieving significant improvement while others experience persistent symptoms. Support from family and friends is important; encouraging treatment adherence and providing a stable environment greatly assist those with schizoaffective disorder.
Related disorders include schizophrenia, bipolar disorder, and major depressive disorder, all of which share overlapping symptoms but differ in their specific presentations and treatment approaches.
What is Schizoaffective Disorder?
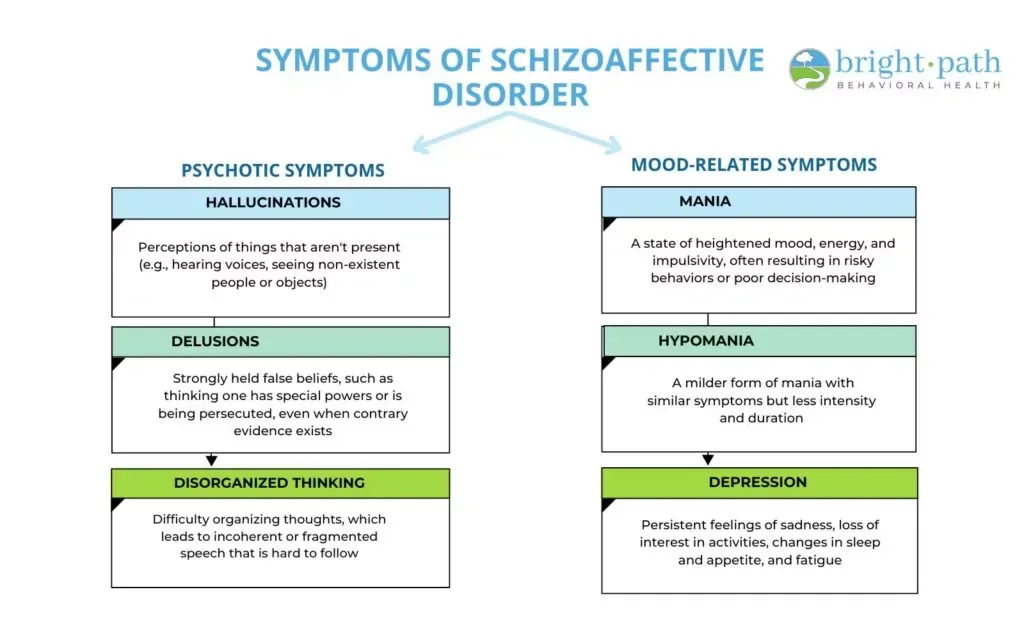
Schizoaffective disorder is a mental health condition that combines symptoms of schizophrenia, such as hallucinations and delusions, with mood disorder symptoms, including depression or mania. This disorder affects how individuals think, feel, and behave, leading to significant challenges in daily functioning and social interactions. It is important to note that schizoaffective disorder is not classified as a personality disorder; rather, it falls under the category of psychotic disorders, which feature both mood disorder symptoms and psychotic symptoms.
There are two main types of schizoaffective disorder: the bipolar type and the depressive type. The bipolar type includes episodes of mania or hypomania along with depressive episodes, where individuals experience elevated mood and increased energy during manic phases, contrasted with feelings of sadness and hopelessness during depressive episodes. In contrast, the depressive type is characterized solely by major depressive episodes without manic or hypomanic episodes, leading to persistent depressive symptoms alongside psychotic experiences.
Among those diagnosed with schizoaffective disorder, around 1 in 150 adults, equating to roughly 40 million individuals or 0.53% of the global population, were living with bipolar type. This condition is predominantly found in working-age individuals, but it also affects younger people, per research published in the World Health Organisation in 2024 titled “Bipolar disorder.”
The term “schizoaffective disorder” was first introduced in the early 20th century, with significant contributions from psychiatrist Jacob Kasanin in 1933, who recognized the co-occurrence of schizophrenia and mood disorder symptoms in some patients. Schizoaffective disorder is estimated to affect about 0.3% of the population, which translates to approximately 3 in every 1,000 individuals, based on research published in Cleveland Clinic in 2023 titled “Schizoaffective Disorder.”
What Are the Symptoms of Schizoaffective Disorder?
The symptoms of schizoaffective disorder include a combination of psychotic symptoms and mood-related symptoms, which significantly affect an individual’s daily life and relationships. These symptoms are explained below:
What Causes Schizoaffective Disorder?
The causes of schizoaffective disorder include genetic, neurobiological, and environmental elements. Here are the primary causes associated with this disorder:
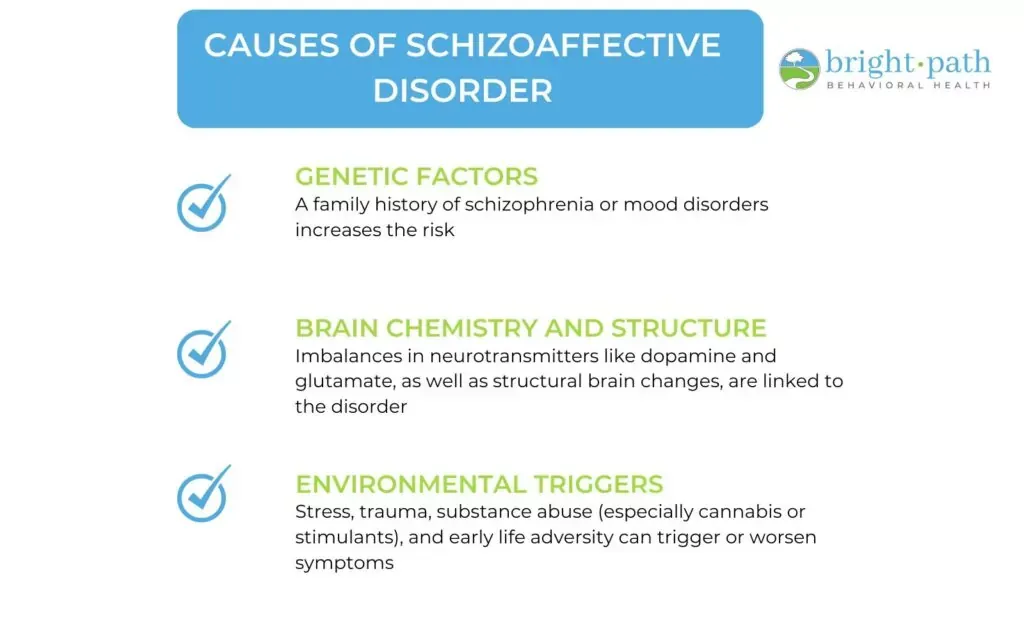
- Genetic Factors: Family history plays a role in the risk of developing schizoaffective disorder. Individuals with first-degree relatives who have schizophrenia or mood disorders are at a higher risk of developing the schizoaffective disorder themselves, according to studies published by MedlinePlus in 2018 titled “Schizoaffective Disorder.”
- Brain Chemistry and Structure: Abnormalities in neurotransmitter systems, particularly involving dopamine and glutamate, are thought to contribute to the symptoms of schizoaffective disorder. These neurotransmitters are crucial for regulating mood and perception. Additionally, structural brain abnormalities, such as changes in the size of certain brain regions, have been observed in individuals with this disorder.
- Environmental Triggers: Various environmental factors trigger or exacerbate symptoms of schizoaffective disorder. Stressful life events, substance abuse (particularly cannabis and stimulants), and trauma during childhood or adolescence are significant contributors. Research has shown that individuals who experience high levels of stress or trauma are more likely to develop psychotic symptoms, and substance use further increases this risk.
Can LSD, Trauma, PTSD, or Drug Use Cause Schizoaffective Disorder?
Yes, trauma, drug use, and other factors contribute to the onset or exacerbation of schizoaffective disorder. While these elements do not directly cause the disorder, they trigger or intensify symptoms in individuals who are already predisposed to mental health issues. People with a history of trauma, particularly during childhood, are at a greater risk for developing various psychiatric disorders, including schizoaffective disorder. A 2016 study by psychosociologist, C Benjet., et al published in Psychological Medicine Journal titled “The epidemiology of traumatic event exposure worldwide: results from the World Mental Health Survey Consortium”, involving general population surveys from 24 countries, with a total of 68,894 adult respondents across six continents, assessed exposure to 29 types of traumatic events. The findings revealed that over 70% of participants reported experiencing at least one traumatic event, while 30.5% were exposed to four or more events. The psychological impact of traumatic experiences leads to the emergence of psychotic symptoms, as trauma disrupts normal emotional and cognitive functioning.
Drug use, especially the use of hallucinogens like Lysergic Acid Diethylamide (LSD), also precipitates psychotic episodes. Although LSD is not a direct cause of schizoaffective disorder, it triggers severe symptoms in individuals who have an underlying vulnerability to such conditions. For example, studies have shown that individuals who use hallucinogens experience psychotic symptoms that resemble those of schizophrenia or schizoaffective disorder, particularly if they have a family history of mental illness.
Furthermore, individuals with Post-traumatic Stress Disorder (PTSD) exhibit symptoms that overlap with those of schizoaffective disorder, such as intrusive thoughts and emotional dysregulation. This overlap complicates diagnosis and treatment, as the presence of PTSD exacerbates the mood-related symptoms of schizoaffective disorder.
What Triggers Schizoaffective Episodes?
Schizoaffective episodes are triggered by drug use, stress, lack of treatment, and major life changes. The common triggers that lead to episodes and exacerbate symptoms are given below:
- Stress: High levels of stress from life events, such as job loss, relationship issues, or significant changes, trigger schizoaffective episodes. Stressful situations exacerbate symptoms and lead to a decline in mental health.
- Drug use: The use of substances, including alcohol and recreational drugs, precipitate or worsen episodes. Drugs alter brain chemistry and trigger symptoms, particularly in individuals with a predisposition to mental health disorders. Roughly 50% of individuals with a substance use disorder also experience co-occurring mental health disorders, such as depression, anxiety, or schizophrenia, according to a study by Jeanne Segal, Ph.D., et al published in Help Guide in 2024 titled “Dual Diagnosis: Substance Abuse and Mental Health.” This high rate of comorbidity emphasizes the complex relationship between substance use and mental health.
- Lack of treatment: Inconsistent or inadequate treatment leads to a resurgence of symptoms. When individuals do not adhere to their prescribed medication or therapy, the risk of experiencing episodes increases.
- Sleep disturbances: Poor sleep quality or insomnia triggers episodes, as sleep is critical for mental health stability. Lack of rest exacerbates mood swings and psychotic symptoms.
- Major life changes Events such as moving to a new location, starting or losing a job, or experiencing the death of a loved one act as triggers, leading to increased anxiety and potential episodes.
The cyclical nature of schizoaffective disorder means that these triggers lead to episodes that, once they occur, further complicate an individual’s ability to manage their condition. For example, a stressor leads to a psychotic episode, which in turn creates additional stress, perpetuating a cycle of worsening symptoms and increased difficulty in treatment.
How is Schizoaffective Disorder Diagnosed?
Schizoaffective disorder is diagnosed by a psychiatrist through a comprehensive process that typically follows the criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). The diagnosis begins with a thorough clinical interview, where a mental health professional assesses the individual’s symptoms, history, and functioning.
The DSM-5 criteria for schizoaffective disorder requires the presence of a major mood episode (either depressive or manic) concurrent with symptoms of schizophrenia. This means that the individual must experience symptoms such as hallucinations or delusions for at least two weeks in the absence of mood symptoms. The mood symptoms must also be present for a substantial portion of the illness.
To support the diagnosis, various tests and assessments are conducted. A psychological evaluation is important, allowing the clinician to gather detailed information about the individual’s mental health history and current symptoms. While there are no specific blood tests or brain scans that definitively diagnose schizoaffective disorder, these tests are used to rule out other medical conditions or to assess overall brain health. For example, brain imaging techniques like MRI or CT scans help identify any structural abnormalities.
As for quizzes, there are online screening tools and self-assessment quizzes available that help individuals gauge their symptoms and determine whether they should seek professional evaluation. However, these quizzes are not diagnostic tools and should not replace a thorough assessment by a qualified mental health professional. If someone suspects they have schizoaffective disorder, it is important to consult with a healthcare provider for an accurate diagnosis and appropriate treatment.
What is the Age of Onset for Schizoaffective Disorder?
The age of onset for schizoaffective disorder begins in late adolescence or early adulthood, with the most common onset occurring between the late teens and the mid-30s, according to a research published by Veteran Affairs titled “Facts About Schizoaffective Disorder.” Specifically, many individuals begin to show symptoms in their late teens to early 20s, although some cases emerge later in life. Various factors influence the age of onset, including genetic predisposition, environmental stressors, and the presence of other mental health conditions.
There are notable differences in the age of onset between men and women. Men experience symptoms earlier, typically in their late teens to early 20s, while women tend to develop symptoms later, in their late 20s to early 30s. This difference in timing is related to hormonal factors and life stressors unique to each gender.
Early intervention is vital in managing schizoaffective disorder and significantly impacts prognosis. When symptoms are recognized and treated promptly, individuals have a better chance of achieving stable recovery and improving their overall quality of life. Early treatment helps mitigate the severity of symptoms and reduce the likelihood of future episodes, emphasizing the importance of awareness and timely access to mental health care.
Can Schizoaffective Disorder Be Misdiagnosed?
Yes, schizoaffective disorder can be misdiagnosed due to its complex symptomatology, which overlaps significantly with other mental health disorders, particularly schizophrenia and bipolar disorder. The difficulty in diagnosis arises from the presence of both mood and psychotic symptoms, which lead to confusion in clinical assessment.
One common pitfall is the tendency to diagnose individuals based solely on their predominant symptoms at the time of evaluation. For instance, if a person presents primarily with manic or depressive symptoms, they are diagnosed with bipolar disorder without adequate consideration of any concurrent psychotic features. Conversely, if psychotic symptoms are more prominent, the individual is misdiagnosed with schizophrenia, especially if mood symptoms are not evident during the assessment.
Another challenge is that the duration and timing of symptoms are essential for an accurate diagnosis. Schizoaffective disorder requires a significant overlap of mood symptoms with psychotic symptoms, but if these criteria are not carefully evaluated, psychiatrists overlook the nuances that distinguish schizoaffective disorder from its counterparts. Additionally, factors such as the individual’s history, the context of symptom presentation, and the use of substances further complicate the diagnostic process.
Misdiagnosis leads to ineffective treatment strategies and worsens the individual’s condition. Therefore, mental health professionals need to conduct thorough assessments, including detailed interviews and consideration of the individual’s entire symptom history, to arrive at an accurate diagnosis and provide appropriate interventions.
What are the Treatment Options for Schizoaffective Disorder?
The treatment options for schizoaffective disorder include medications, psychotherapy, and lifestyle and support. Schizoaffective disorder is hard to treat due to its dual nature, involving both mood and psychotic symptoms. The overlapping symptoms of schizophrenia and bipolar disorder complicate diagnosis and treatment, leading to potential misdiagnosis and ineffective treatment strategies. Also, individual responses to medications vary widely, necessitating a tailored approach to treatment.
The treatment options for schizoaffective disorder include:

1. Medications
Medications are the cornerstone of treatment for schizoaffective disorder, helping to stabilize mood and manage psychotic symptoms. A combination of different types of medications is used to address the diverse range of symptoms that individuals experience. These medications include:
- Antipsychotics: These are the first line of treatment for managing psychotic symptoms. Commonly prescribed antipsychotics include paliperidone, risperidone (Risperdal), and olanzapine (Zyprexa).
- Mood Stabilizers: These are particularly important for individuals with the bipolar type of schizoaffective disorder. Examples include lithium and valproate (Depakote).
- Antidepressants: When depressive symptoms are prominent, antidepressants are prescribed to alleviate feelings of sadness and hopelessness. Common options include Selective Serotonin Reuptake Inhibitors (SSRIs) such as fluoxetine (Prozac) or sertraline (Zoloft).
The best medicine for schizoaffective disorder varies by individual, but a combination of antipsychotics and mood stabilizers or antidepressants is most effective in managing symptoms.
2. Psychotherapy
Psychotherapy plays an important role in the treatment of schizoaffective disorder, providing individuals with tools to cope with their symptoms, improve interpersonal relationships, and enhance their overall functioning. Various therapeutic approaches are beneficial.
- Cognitive Behavioral Therapy (CBT): This therapy helps individuals identify and change negative thought patterns and behaviors. It has been shown to be effective in reducing symptoms and improving coping strategies, according to research published in Cleveland Clinic in 2023 titled “Schizoaffective Disorder.”
- Family Therapy: Family therapy involves family members in the treatment process to improve communication and support within the family unit. This approach helps reduce stress and improve the overall functioning of the individual with schizoaffective disorder.
- Social Skills Training: Social skills training focuses on improving interpersonal skills and daily functioning. This training helps individuals better navigate social situations and improve their quality of life.
3. Lifestyle and Support
In addition to medications and therapy, lifestyle changes and support systems are essential for effective management of schizoaffective disorder. These components enhance overall well-being and provide ongoing support. They include:
- Lifestyle Changes: Incorporating regular exercise, a balanced diet, and good sleep hygiene significantly improves overall well-being and helps manage symptoms. Stress management techniques, such as mindfulness and relaxation exercises, are also beneficial.
- Support Groups: Connecting with others who have similar experiences provides emotional support and practical advice. Support groups help reduce feelings of isolation and promote recovery.
- Ongoing Care: Regular follow-ups with healthcare providers are essential for monitoring symptoms and adjusting treatment as necessary. Developing a strong support network, including friends, family, and mental health professionals, is crucial for the effective management of the disorder.
Can Schizoaffective Disorder Be Cured?
No, schizoaffective disorder cannot be cured, but it is a manageable condition. The prognosis for individuals with schizoaffective disorder varies; while some experience chronic symptoms, many lead fulfilling lives with appropriate treatment and support. Up to 81.9% of people with schizoaffective disorder experience a relapse within five years of their diagnosis. This high rate of relapse is due to the chronic nature of the illness, as highlighted by research conducted by Anne R. et al., published in 2024 in Nature, titled “Real-world predictors of relapse in patients with schizophrenia and schizoaffective disorder in a large health system.”
Management of schizoaffective disorder typically involves a combination of medications, psychotherapy, and lifestyle changes. With a tailored treatment plan, individuals stabilize their symptoms, reduce the frequency and severity of episodes, and improve their overall quality of life. Early intervention and ongoing support are essential in helping individuals deal with the challenges of the disorder.
Emphasizing management over the idea of a cure is important, as it allows individuals to focus on their strengths and capabilities rather than solely on their diagnosis. Many people with schizoaffective disorder successfully pursue careers, maintain relationships, and engage in meaningful activities. With the right resources and coping strategies, those affected achieve a high quality of life, demonstrating that living well with schizoaffective disorder is entirely possible.
How to Live with Schizoaffective Disorder?
To live with schizoaffective disorder, you have to learn how to create a routine, prioritize medication adherence, practice stress management, develop coping strategies, communicate openly, seek support, etc.
Practical tips for living with schizoaffective disorder are given below:
- Create a daily schedule that includes regular wake-up and sleep times, meals, and activities. A consistent routine provides structure and stability.
- Take prescribed medications as directed and keep regular appointments with healthcare providers. Discuss any side effects or concerns with your doctor.
- Engage in relaxation techniques such as mindfulness, meditation, or yoga to help reduce stress and anxiety. Exercise regularly to improve mood and overall well-being.
- Identify effective coping mechanisms, such as journaling, deep breathing exercises, or engaging in hobbies, to manage symptoms and emotions.
- Maintain open lines of communication with friends, family, and coworkers about your condition. Educating them about schizoaffective disorder fosters understanding and support.
- Join support groups or connect with others who have similar experiences. Sharing challenges and successes encourages and reduces feelings of isolation.
- Avoid drugs and limit alcohol consumption, as they exacerbate symptoms and interfere with treatment.
By incorporating these strategies into daily life, you will effectively manage your condition and lead a fulfilling life.
How Does Schizoaffective Disorder Affect Daily Life and Relationships?
Schizoaffective disorder significantly impacts daily life and relationships, creating challenges in work, family dynamics, and social interactions. In the workplace, individuals struggle with concentration, memory, and motivation, hindering job performance. Mood swings and psychotic episodes lead to absenteeism, affecting teamwork and communication.
Family life is strained due to misunderstandings about the disorder, with family members feeling frustrated or helpless, leading to conflicts and emotional distance. Educating loved ones about the condition improves understanding and support, fostering healthier relationships.
A feature story published in 2024 by the National Institute of Mental Health titled “Life with Schizoaffective Disorder” showcases Ray Lay’s journey, exemplifying these challenges. After a traumatic childhood accident, he began experiencing hallucinations that led to behavioral changes, misunderstandings, and conflicts with his family. His struggles with untreated symptoms resulted in homelessness and substance abuse, illustrating the severe impact of schizoaffective disorder on daily life. Lay’s experience aligns with findings from a study that highlights how personality traits and symptom severity influence social functioning and relationships in individuals with schizophrenia spectrum disorders, including schizoaffective disorder.
Despite these hurdles, many individuals with schizoaffective disorder maintain employment, particularly in flexible environments that accommodate their needs. In terms of love and relationships, individuals like Lay form meaningful connections, although challenges remain. Open communication and understanding from partners are essential, as demonstrated by Lay’s eventual recovery and advocacy work. His story highlights the importance of trust and reassurance in strengthening relationships, allowing individuals to express their feelings and needs effectively.
Can Someone with Schizoaffective Disorder Lead a Normal Life?
Yes, someone with schizoaffective disorder can lead a normal life. With proper treatment, many people function normally in most aspects of life, including work, relationships, and social activities. Treatment involves a combination of medication, psychotherapy, and lifestyle adjustments, which helps manage symptoms effectively.
Modern treatment options have improved significantly, allowing individuals to achieve better outcomes. For instance, coordinated specialty care approaches that include medication management, psychotherapy, and support services have helped a lot of people with schizoaffective disorder lead fulfilling lives.
Moreover, individuals who actively engage in their treatment plans and maintain a healthy lifestyle such as regular exercise, a balanced diet, and good sleep hygiene report improved quality of life and better management of their symptoms.
How Severe is Schizoaffective Disorder?
The severity of schizoaffective disorder ranges from mild symptoms to severe cases that are debilitating. The degree of impairment depends on several factors, including treatment adherence, individual triggers, and the presence of co-occurring conditions.
Mild symptoms include occasional mood swings or brief hallucinations, which are managed effectively with outpatient treatment. With proper support, many people maintain a relatively normal daily life. In contrast, more pronounced symptoms lead to difficulties in relationships, work, and social situations, making treatment adherence crucial.
Severe cases result in persistent hallucinations, delusions, and significant functional impairment, requiring hospitalization and intensive treatment. Co-occurring disorders, such as anxiety or substance use disorders, complicate the treatment and management of schizoaffective disorder. These conditions can interact with the primary disorder, leading to increased symptom severity and challenges in achieving stability, per a study published in the National Alliance on Mental Illness in 2023 titled “Schizoaffective Disorder.”
What is the Prognosis of Schizoaffective Disorder?
The prognosis of schizoaffective disorder is influenced by early and consistent treatment, which significantly improves long-term outcomes and quality of life.
Consistent treatment also enhances the quality of life. Patients who engage in ongoing therapy and medication management report better social functioning and greater satisfaction with life. Those receiving comprehensive care are more likely to maintain employment and live independently.
Additionally, early and ongoing treatment reduces the risk of relapse. Individuals with schizoaffective disorder are particularly vulnerable to relapse, especially in the first few years post-diagnosis. Adherence to treatment regimens is associated with lower relapse rates and reduced healthcare costs, per a study published by Cambridge University Press in 2018 titled “Ten-year outcome: patients with schizoaffective disorders, schizophrenia, affective disorders, and mood-incongruent psychotic symptoms.”
Does Schizoaffective Disorder Get Worse With Age?
Yes, schizoaffective disorder gets worse with age. For some, symptoms worsen with age, particularly if treatment is inconsistent or inadequate. However, with appropriate and consistent treatment, many individuals experience stabilization of symptoms and improved quality of life as they age.
The disorder presents with varying severity at different life stages, and certain triggers, such as stress or substance use, exacerbate symptoms. Research suggests that early intervention and ongoing management are crucial in mitigating potential deterioration.
While some individuals face challenges as they age, others achieve better symptom control and functioning through effective treatment strategies. Overall, the trajectory of schizoaffective disorder is highly individual and depends significantly on factors such as adherence to treatment and availability of support systems.
What is the Life Expectancy of Someone with Schizoaffective Disorder?
A 2011 study indicated that the average life expectancy at birth for individuals with schizoaffective disorder is 69.4 years for men and 64.1 years for women. This represents a reduction of 8 years for men and 17.5 years for women compared to the general population’s average life expectancy, as indicated in a study by Chang et al., published in PLOS ONE in 2011 titled “Life Expectancy at Birth for People with Serious Mental Illness and Other Major Disorders from a Secondary Mental Health Care Case Register in London.”
Individuals with schizoaffective disorder face higher rates of comorbid conditions such as cardiovascular disease, diabetes, and substance use disorders, which increase health risks. These comorbidities complicate treatment and lead to further health complications.
Lifestyle choices also play a critical role in longevity. Poor diet, lack of exercise, and substance abuse contribute to health issues while maintaining a healthy lifestyle improves overall well-being.
Access to consistent treatment is essential for managing symptoms and reducing complications. Those who receive appropriate care, including medication and therapy, generally experience better outcomes.
Life expectancy improved for individuals with serious mental illnesses, including schizoaffective disorder, yet remained lower than that of the general population, according to one study by health researcher, Alyson P. K., published in WebMD in 2024 titled “Schizoaffective Disorder: Causes, Signs, Treatment.”
How to Help a Loved One With Schizoaffective Disorder?
To help a loved one with schizoaffective disorder, you have to involve a combination of emotional support, empathy, patience, and encouraging professional help.
Here are some practical strategies for families and caregivers:
- Learn about the symptoms, treatment options, and potential challenges. This knowledge helps you respond effectively and compassionately.
- Show empathy and be there for your loved one. Listen actively and validate their feelings without judgment. Let them know they are not alone in their struggles.
- Support your loved one in adhering to their treatment plan, including medication and therapy. Offer to accompany them to appointments or help with medication reminders.
- Establish a calm and predictable home environment. Routines provide structure, which helps reduce anxiety and stress for your loved one.
- Encourage a balanced diet, regular exercise, and sufficient sleep. These factors significantly impact mental health and overall well-being.
- Help your loved one maintain social connections. Encourage participation in activities they enjoy, but be mindful of their comfort levels and triggers.
How to Talk to Someone with Schizoaffective Disorder?
To talk to someone with schizoaffective disorder requires patience and support. Below are some do’s and don’ts for communicating effectively with someone who has schizoaffective disorder, focusing on empathy and avoiding triggers:
Do’s
- Use simple, clear language to avoid misunderstandings.
- Listen actively and show genuine interest in what they are saying.
- Validate their feelings and experiences, even if you don’t fully understand.
- Be patient and give them time to express themselves.
- Maintain a calm and reassuring tone, especially during difficult conversations.
- Offer support without pushing them to share more than they are comfortable with.
- Encourage them to seek professional help if they express distress or confusion.
Don’ts
- Avoid using judgmental or dismissive language that could invalidate their feelings.
- Don’t argue or challenge their perceptions or beliefs directly.
- Refrain from using complex or abstract language that is confusing.
- Don’t interrupt or rush them when they are speaking.
- Avoid discussing sensitive topics that could trigger anxiety or distress.
- Don’t take negative reactions personally; their symptoms influence their responses.
- Avoid making assumptions about their experiences or feelings; ask open-ended questions instead.
- Don’t push them to talk if they seem withdrawn or reluctant.
What Not to Say to Someone with Schizoaffective Disorder?
Here are some phrases to avoid when talking to someone with schizoaffective disorder, along with supportive alternatives:
What Not to Say
By avoiding these harmful phrases and using supportive alternatives, you create a more compassionate and understanding environment for someone with schizoaffective disorder.
What Can Be Mistaken for Schizoaffective Disorder?
Several mental health conditions are mistaken for schizoaffective disorder due to overlapping symptoms. Schizophrenia shares similarities, particularly in psychotic features such as hallucinations and delusions, but lacks the prominent mood symptoms found in schizoaffective disorder.
Bipolar disorder also presents with episodes of mood disturbance and psychotic features, making it difficult to differentiate, especially during manic or depressive phases. Additionally, major depressive disorder with psychotic features is confused with schizoaffective disorder when mood symptoms are significant.
Accurate diagnosis requires careful assessment by a mental health professional to distinguish between these conditions based on the presence and duration of mood symptoms alongside psychotic experiences.
What is the Difference Between Schizoaffective Disorder and Schizophrenia?
The difference between schizoaffective disorder and schizophrenia is primarily in the nature and duration of symptoms. While schizoaffective disorder and schizophrenia share some similarities, they have distinct characteristics that set them apart. The following comparison highlights key aspects of each disorder, including their definitions, symptoms, treatment options, and prognosis.
The severity of each condition varies by individual; schizoaffective disorder involves more significant mood fluctuations, while schizophrenia presents more persistent psychotic symptoms.
What is the Difference Between Bipolar Disorder and Schizoaffective Disorder?
Bipolar disorder and schizoaffective disorder share similarities, particularly in the presence of mood episodes and psychotic features, but they are distinct conditions. Bipolar disorder is characterized by extreme mood swings, including manic episodes (elevated mood, increased energy) and depressive episodes, without the requirement of psychotic symptoms. Individuals with bipolar disorder can experience significant mood changes without necessarily having hallucinations or delusions during their episodes according to a research published by the NIH in 2022 titled “Bipolar Disorder.”
In contrast, schizoaffective disorder includes both mood disturbances and psychotic symptoms, such as hallucinations and delusions, that occur independently of mood episodes. While individuals with schizoaffective disorder experience mood symptoms, the defining feature is the presence of psychosis that persists even when mood symptoms are not active.
This overlap complicates diagnosis, making it essential for mental health professionals to assess the timing and nature of symptoms carefully.
Is Schizoaffective Disorder a Disability?
Yes, schizoaffective disorder qualifies as a disability under Social Security Administration (SSA) guidelines. According to the SSA, it is recognized as a severe mental disorder that significantly impairs an individual’s ability to function in daily life and work. To qualify for disability benefits like Supplemental Security Income (SSI), applicants must provide medical documentation demonstrating the severity of their condition, including symptoms and treatment history.
The SSA evaluates schizoaffective disorder under the category of “schizophrenia spectrum and other psychotic disorders,” which requires evidence of significant functional limitations and the presence of psychotic symptoms Additionally, to meet the criteria for a serious and persistent mental disorder, there must be a documented history of the disorder over a period of at least two years.
To apply for SSI, individuals should gather relevant medical records and treatment histories that detail their diagnosis and its impact on daily functioning. The application is submitted online, by phone, or in person at a local SSA office. The SSA requires a consultative examination to assess the applicant’s condition further.
After applying, it takes several months to receive a decision. If approved, benefits will help cover basic living expenses. If denied, applicants have the right to appeal the decision. Providing accurate information is essential for improving the chances of receiving benefits. Consulting with a legal expert or advocate specializing in disability claims is also helpful.